

The most recent nutrition and IBD guidelines from the European Society for Clinical Nutrition and Metabolism (ESPEN) recommend regular screening for micronutrient deficiencies in IBD patients and correcting any identified deficits, even in those who appear well-nourished or are in remission.
What could be causing micronutrient deficiencies in IBD patients?

Current literature suggests that over 50% of patients with IBD have had at least 1 vitamin or mineral deficiency.
Micronutrient absorption occurs mostly across the epithelium of the small intestine, which is likely why patients with Crohn’s disease (CD) have a higher prevalence of nutritional deficiencies compared with those with ulcerative colitis (UC).
The most common micronutrient deficiencies are:
- Vitamins: Vitamin C, Vitamin D, Vitamin B6, Vitamin B9, and Vitamin B12
- Minerals: Iron, Zinc, Magnesium, and Calcium
The tables below indicate the most common nutritional deficiencies, their sources, effects, and causes.
Table 1 : Common Vitamin Deficiencies in IBD Patients: Causes, Effects, and Sources
| Vitamin | Sources | Deficiency Effects | Causes |
|---|---|---|---|
 Vitamin B6 | Fish, poultry, legumes, potatoes | Depression, anxiety, anemia, mouth ulcers/cracks | Inflammation in the small intestine due to Crohn’s disease. |
 Vitamin B9 | Leafy greens, avocado, whole grains, legumes | Anemia, increased risk of colon cancer | Avoidance of high- fiber foods, use of medications (e.g., sulfasalazine or methotrexate), resection or inflammation in the small intestine, low stomach acid levels. |

Vitamin B12 | Meat, fish, eggs, dairy products | Anemia, tingling in hands/feet, fatigue, memory problems, cognitive decline | Crohn’s disease affecting the ileum, surgical removal of the ileum, strict vegetarian diets. |
 Vitamin C | Citrus fruits, tomatoes, strawberries, bell peppers | Joint pain, anemia, fatigue, edema, mouth ulcers, bleeding gums, poor wound healing | Avoidance of fresh fruits and vegetables during disease flares. |
 Vitamin D | Fortified milk, sunlight, fatty fish (e.g., salmon, sardines) | Weak bones, increased risk of osteoporosis | Chronic use of corticosteroids, small intestinal inflammation, small intestine resection, bacterial overgrowth in the small intestine. |
Table 2: Common Mineral Deficiencies in IBD Patients: Causes, Effects, and Sources
| Mineral | Sources | Deficiency Effects | Causes |
|---|---|---|---|

Calcium | Dairy products, leafy green vegetables | Low bone density, hyperparathyroidism, high blood pressure, muscle cramps | Small intestinal inflammation, vitamin D deficiency, corticosteroid use for over 3 months |

| Red meat, legumes, whole grains | Anemia, fatigue, poor focus, infertility in women | Chronic blood loss, impaired iron metabolism, insufficient dietary intake |
 Zinc | Poultry, meat, seafood, nuts, legumes, whole grains | Changes in taste or smell, delayed wound healing, hair loss, night blindness, stunted growth | Crohn’s disease with abscesses, chronic diarrhea, small intestine resection, corticosteroid use |

Magnesium | Nuts, peanut butter, legumes, whole grains, leafy greens | Sleep disturbances, anxiety, heart rhythm disorders, muscle spasms | Small intestine inflammation or resection, chronic diarrhea, fistulas |
Location Matters!
Inflammation or surgical removal of parts of the gastrointestinal tract, especially the small intestine, can lead to deficiencies in certain micronutrients. This is because the inflammation or surgical removal can damage absorption sites, increasing the chances of micronutrient deficiencies.

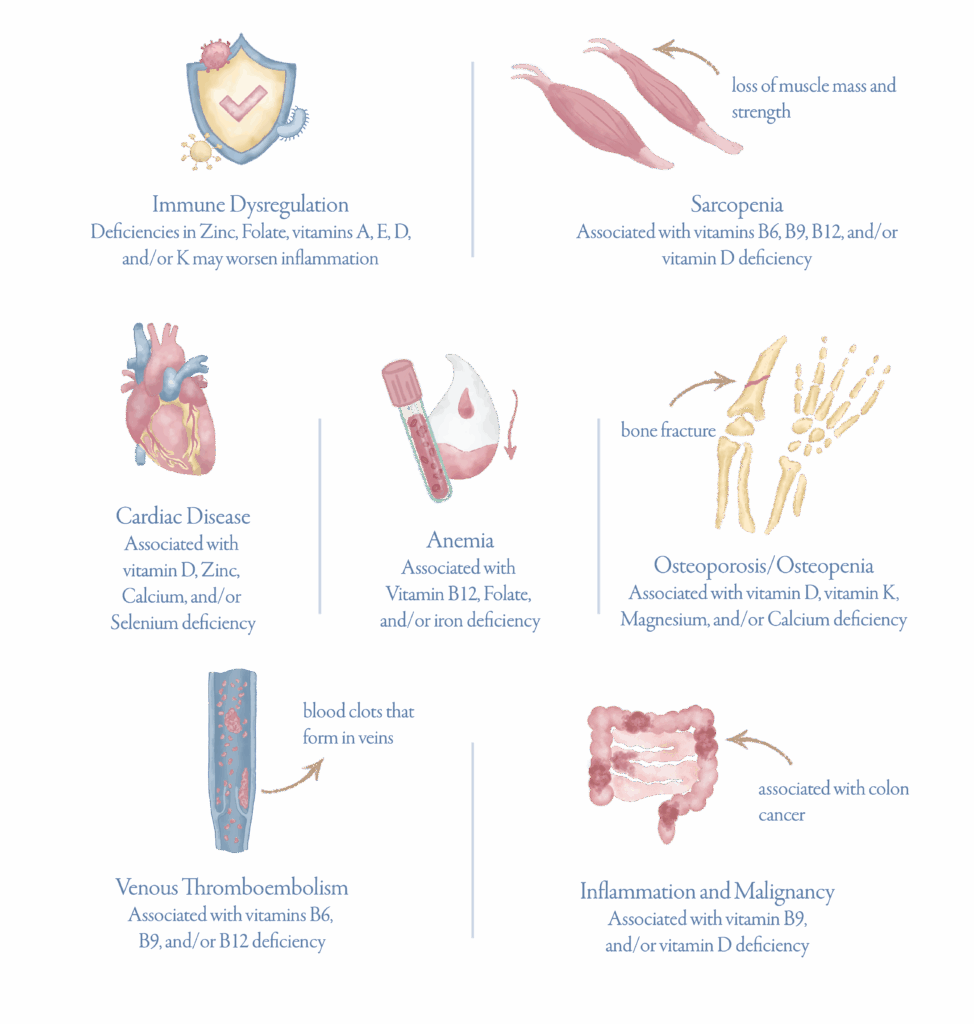
Untreated micronutrient deficiencies can lead to a wide-range of health problems causing the following:
Patients with inflammatory bowel disease (IBD), like Crohn’s disease and ulcerative colitis, are at high risk of developing micronutrient deficiencies due to a variety of factors, including malabsorption from intestinal inflammation and increased nutrient needs during disease activity.
Crohn’s patients tend to be at higher risk than those with ulcerative colitis, especially if the disease affects the small intestine where many nutrients are absorbed. Removing parts of the intestines can also increase deficiency risk.
Deficiencies in vitamins and minerals can contribute to serious symptoms and complications including an increased risk of bone disease, anemia, malignancies and others.
That’s why regular screening and intervention is crucial, even for those in remission. Remember that understanding the location of your IBD and monitoring your micronutrient status is key to staying healthy. Talk to your doctor about getting the right testing and supplementation.
References
- Bischoff SC, Bager P. Escher J. Forbes A, Hébuterne X. Hvas CL, Joly F. Klek S. Krznaric Z. Ockenga J. Schneider S. Shamir R, Stardelova K, Bender DV, Wierdsma N, Weimann A. ESPEN guideline on Clinical Nutrition in inflammatory bowel disease. Clin Nutr. 2023 Mar:42(3):352-379.
- Chiu E. Oleynick C, Raman M. Bielawska B. Optimizing Inpatient Nutrition Care of Adult
Patients with Inflammatory Bowel Disease in the 2lst Century. Nutrients. 2021 May 9:13(5) 1581. - Gold SL, Manning L, Kohler D. Ungaro R, Sands B, Raman M. Micronutrients and Their Role in
Inflammatory Bowel Disease: Function, Assessment, Supplementation, and Impact on Clinical
Outcomes Including Muscle Health. Inflamm Bowel Dis. 2023 Mar 129(3:487-501. - Li X, Hu Y, Shi X, Zhu X, Liu F. Prevalence and relevant factors of micronutrient deficiencies in hospitalized patients with inflammatory bowel disease. Nutrition. 2022 Jul-Aug: 99-100:111671.
- Weisshof R, Chermesh I Micronutrient deficiencies in inflammatory bowel disease. Curr Opin Clin Nutr Metab Care. 2015 Nov:18(6)576-81.





